


June 2025
50/50: Appreciating the Nuance of
Local Markets
Table of Contents






Appreciating the Nuance of Local Markets
Homogony and malpractice insurance are antonyms. There is no end to the differences in regulations, levels of volatility, legislative actions, licensing requirements, and the like which vary from state to state (if not county!). It may be challenging, but it’s also half the fun.
After all, as we are fond of saying (compliments of former ProAssurance CEO Stan Starnes) “If you’re in 50 states, you’re in 50 different lines of business.”
No matter the size of your footprint, success is often derived from your ability to drill down into that nuance. Nationwide carriers and agency partners alike need to be able to speak the language of the physician—what is relevant and useful right in their backyard. This isn’t anything new; we’ve been doing it for decades.
But as tort reform heats up and judicial hellholes migrate, the targets of opportunity can shift. Suddenly a state that was an afterthought five years ago is a juicy target in today’s market. Being able to quickly and efficiently understand the landscape in a new territory can make all the difference before heading into a meeting.
That idea spawned our state profiles. Each year, as S&P Global releases their latest market share information for the industry, we begin updating our library so our agency partners can have an easy reference should you need to train new employees—or find yourself asked to evaluate an opportunity in an area outside of your usual territory.
We have included a selection of profiles here in this issue which help to illustrate key differences one might encounter when operating with a national med-mal footprint—but the full library is available and being updated on our agent website. Feedback is always appreciated, so if there is additional information you would find helpful in our profiles, send your suggestions to AskMarketing@ProAssurance.com.

Topping the Charts
Operating in 50 states is a feat in and of itself but establishing a solid presence in those states is far more essential for long-term success. ProAssurance is ranked as a top-three medical malpractice insurer by market share in 13 states, and a top-ten ranked carrier in 40 states. See the full map on our About Us page.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
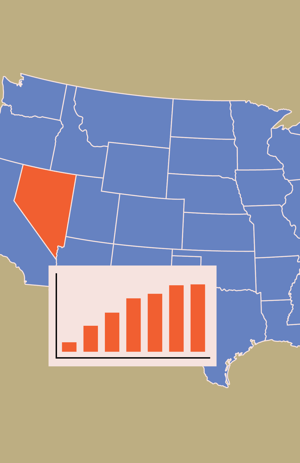
Physician Market Comparison
Nevada = $69,084,099
About the same as Kentucky ($68,419,561)
Virginia is about twice the size ($139,417,623)
Iowa is about half the size ($36,980,505)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: $510,000 noneconomic damages cap (increases $80k on 1/1 through 2028, then 2.1% annual inflation adjustment)- Rev. Stat. Ann. § 41A.035
- Rev. Stat. Ann. § 7.095
- Rev. Stat. Ann. § 42.021
- Rev. Stat. Ann. § 42.021
- Rev. Stat. Ann. § 41A.097
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: If the rate is not established by contract, a rate equal to the prime rate at the largest bank in Nevada, plus 2%.- Rev. Stat. Ann. § 17.130
- Rev. Stat. Ann. § 17.130
- Rev. Stat. Ann. §§ 99.050; 17.130(2)
Recording Consent
Nevada is a mixed-party consent state.
In Nevada, it is a criminal offense to use any device to record, obtain, share or use oral conversations without the consent of at least one person taking part in the communication. However, the recording or sharing of wire conversations require the consent of all involved parties. This means that in Nevada, you are legally allowed to record an oral conversation if you are a contributor, or with prior consent from one of the involved parties, but you need the consent of everyone involved to record wire communications. Wired communication refers to the transmission of data, so even if it's a wireless device such as a cellphone it is still considered to be wired communication. Examples of wired communications are cell phones, land lines, zoom calls, and VOIP. Nev. Rev. Stat. Ann. §§ 200.620, 200.650
Abortion Law
Abortion will remain legal in Nevada. In 1990, Nevada voters passed a referendum safeguarding the state’s law legalizing abortion, and, in 2024 voters approved an amendment to the Nevada Constitution to protect abortion rights, which requires a second vote in 2026 to be effective.
CME Requirements
- For MDs, Nevada requires 40 CME hours per licensure cycle. Physicians licensed for less than the full cycle will follow prorated CME credit requirements.
- For DOs, Nevada requires 35 CME hours per licensure cycle.
- 20 hours per licensure cycle within the scope of practice or specialty
- 2 hours per licensure cycle pertaining to ethics, pain management, or addiction care
- 2 hours per licensure cycle of CME on the subject of controlled substances, prescribing opioids, or addiction
- 2 hours every 4 years of education about suicide detection, intervention, and prevention
- 2 hours of CME annually on the topic of substance abuse of controlled substances, the prescribing of opioids, or addiction
- 2 hours of CME in even-numbered years only pertaining to ethics, pain management, or addiction care
- 2 hours of evidence-based suicide prevention and awareness education is due within 2 years, then 2 hours every 4 years
The state CME requirements listed above were accurate when posted, but CME state requirements change frequently. Due to COVID-19, certain states may have modified their licensure requirements. Physicians are advised to confirm requirements with the Nevada State Board of Medical Examiners website and the Nevada State Board of Osteopathic Medicine website.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Delaware = $25,493,816
About the same as Maine ($24,373,455)
Louisiana is about twice the size ($50,493,069)
Wyoming is about half the size ($11,791,020)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Limits on damages for pain and suffering: None
Limits on contingent attorney fees: Sliding scale
- Del. Code Ann. tit. 18 § 6865
- Del. Code Ann. tit. 18 § 6862
- Del. Code Ann. tit. 18 § 6864
- Del. Code Ann. tit. 18 § 6856—upheld
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: 5% over the Federal Reserve discount rate- Del. Code Ann. tit. 6, § 2301
- Del. Code Ann. tit. 6, § 2301; see Cumberland Ins. Group v. KCL Enters., 2003 Del. Super. LEXIS 500 (August 26, 2003) (in subrogation cases, the date of injury is the date of each insurance payment)
- Del. Code Ann. tit. 6, § 2301; see Payne v. Home Depot, Inc., 2009 Del. Super. LEXIS 129 (April 7, 2009)
- Del. Code Ann. tit. 6, § 2301; see Payne v. Home Depot, Inc., 2009 Del. Super. LEXIS 129 (April 7, 2009)
Recording Consent
Delaware is a two-party state.
In Delaware, it is a criminal offense to use any device to record communications, whether wire, oral, or electronic, without the consent of all parties taking part in the communication. This means that in Delaware you are not legally allowed to record a conversation you are taking part in unless all parties are in agreement. Del. Code Ann. tit. 11, § 1335(a)(4). Also, Delaware has a law that prohibits anyone from trespassing on private property to eavesdrop or carry out any other form of surveillance. Del. Code Ann. tit. 11, § 1335(a)(1).
Abortion Law
Abortion remains legal in Delaware. State law includes express protections for abortion. In 2021, Delaware repealed its final pre-Roe ban.
CME Requirements
Delaware physicians are required to complete 40 hours of CME per licensure cycle. Physicians who are licensed less than one year are not required to complete CME. Physicians licensed more than one year but less than two years are required to complete 20 hours of CME.
Physicians must complete two CME credit hours in the areas of controlled substance prescribing practices, treatment of chronic pain, or other topics related to the prescribing of controlled substances biennially.
CME requirements listed above were updated based on information from the Delaware Board of Medical Licensure and Discipline, but education requirements do change. Due to COVID-19, certain states may have modified their licensure requirements. Physicians should confirm Delaware’s current requirements provided by the Delaware Board of Medical Licensure and Discipline.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Texas = $195,739,891
About the same as Michigan ($151,134,721)
Illinois is about twice the size ($337,994,942)
Massachusetts is about half the size ($99,065,217)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: $250k cap on non-economic damages per claimant for all physicians; $250k cap on non-economic damages per claimant for institution (up to 2)- Civ. Prac. & Rem. Code Ann. § 74.301
Reform of collateral source rule: None
Periodic payment of future damages: Mandatory at request of plaintiff or defendant
- Civ. Prac. & Rem. Code Ann. § 74.503
- Civ. Prac. & Rem. Code Ann. § 74.251
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: The post judgment interest rate applicable at the time of judgment. Interest is computed as simple interest and does not compound. Prejudgment interest not allowed on punitive damages.- Fin. Code Ann. §§ 304.103; 304.104; Tex. Civ. Prac. & Rem. Code Ann. § 41.007
- Fin. Code Ann. § 304.104
- Fin. Code Ann. § 304.003
- Fin. Code Ann. § 304.005
Recording Consent
Texas is a one-party state.
Texas recording law stipulates that it is a one-party consent state. In Texas, it is a criminal offense to use any device to record or share communications, whether they are wire, oral or electronic, without the consent of at least one person taking part in the communication. This means that in Texas, you are legally allowed to record a conversation if you are a contributor or with prior consent from one of the involved parties, barring any criminal intentions. It is also lawful to record electronic communications that are easily available to the public. Tex. Penal Code Ann. § 16.02.
Abortion Law
Texas is enforcing its trigger ban, which prohibits abortion and includes civil and criminal penalties There is an exception for situations in which the life or health of the patient is at risk.
CME Requirements
24 of the 48 required credit hours must be earned from courses or programs that are Category 1 or Category 1A CME with the following topical requirements: 2 hours of Category 1 or Category 1A CME on medical ethics and/or professional responsibility; 2 hours of Category 1 or Category 1A CME on alternative pain management treatment options and/or opioid and controlled substance prescribing and monitoring, and completion of a human trafficking prevention course.
CME requirements listed above were updated based on information from the Texas Medical Board (TMB), but education requirements do change. Due to COVID-19, certain states may have modified their licensure requirements. Physicians should confirm Texas' current requirements on the TMB's Continuing Medical Education for MDs/DOs page.

State Compensation Funds: What You Need to Know
A patient compensation fund (PCF), as the name suggests, helps to ensure reasonable compensation for patients who have been injured due to medical negligence. These funds were legislative responses to the medical malpractice crisis of the 1970s that saw several cascading factors threatening instability in the medical liability market. As state tort laws became more favorable to plaintiffs, plaintiff attorneys recognized the opportunities presented by medical malpractice lawsuits, especially in an environment of increasingly complex medicine.1
These factors contributed to a rapidly diminishing market for providers seeking liability insurance which, at the time, was sold as a separate line by traditional commercial carriers. Out of this crisis came the legislative response of PCFs and new companies specializing in medical malpractice insurance—the industry we now know as medical professional liability insurance.1
The compensation available under a PCF is in excess of underlying coverage obtained by eligible healthcare providers from their liability insurers. The funds also generally limit a provider’s liability to a specific amount. At the time the funds were created, they were seen as an effective way of increasing accessibility to medical malpractice insurance at a reasonable cost.2
Which States Operate Patient Compensation Funds?
Seven states currently operate patient compensation funds, with many funded by surcharges on the underlying coverage. They vary by state on features such as provider eligibility, coverage details, surcharges, residency requirements, requirements for underlying coverage, and more. Provider participation in these funds also varies by state. It is mostly voluntary in Indiana, Louisiana, Nebraska, and New Mexico, while in Kansas, Pennsylvania, and Wisconsin participation is largely mandatory for most providers.
The table below provides a general state-by-state summary of the key details of these funds.
The information here is for general understanding only. Visit the fund website for specific details about a fund.
| Fund Website | Indiana Patient’s Compensation Fund | Kansas Health Care Stabilization Fund | Louisiana Patient’s Compensation Fund | Nebraska Excess Liability Fund | New Mexico Patient’s Compensation Fund | Pennsylvania Medical Care Availability and Reduction of Error Fund | Wisconsin Injured Patients and Families Compensation Fund |
| Mandatory or Voluntary? | Voluntary for most entities and individuals practicing in IN (residents and non-residents) | Mandatory for most healthcare providers practicing in KS (residents and non-residents) | Voluntary for providers practicing in LA (residents and non-residents) | Voluntary for providers practicing in NE (residents and non-residents) | Voluntary for covered providers practicing in NM (residents and non-residents) | Mandatory for most providers practicing in PA (residents and non-residents) | Mandatory for most providers who practice in WI >240 hrs/yr and most providers who are WI residents but practice in MI; voluntary for other providers |
| Fund Limits* | Total cap of $1,650,000 for act of malpractice between 6/30/17 and 7/1/19; $1,800,000 thereafter Provider capped at $400,000 from 6/30/17 to 7/1/19; $500,000 thereafter |
Multiple options available | Total cap on damages is $500,000 (exclusive of medical costs, which are paid by the fund); provider only liable for $100,000 | $2,250,000 total cap | $750,000 total cap for individual providers who belong to the fund, except for medical care and punitive damages. Provider capped at $250,000 |
$500,000/ $1,500,000 for individual providers |
No limit. The Fund indemnifies its participants for any amount over $1,000,000 |
| Coverage Type | Claims Made or Occurrence | Claims Made | Claims Made or Occurrence | Claims Made or Occurrence based on underlying coverage | Occurrence | Underlying coverage may be Claims Made or Occurrence, but MCARE coverage is occurrence only. | Occurrence |
| Does Fund coverage extend outside of the Fund state? | No |
If KS resident, yes. Coverage is worldwide. If contributing as a non-resident, coverage is limited to KS. |
No | No | No | Yes, it follows the physician if they have incidental coverage in another state covered by their PA policy. | Yes, if the primary practice is in WI. |
| Who submits information to the Fund? | Carrier | Carrier | Carrier | Insured | Insured | Carrier | Carrier |
* Limits are in excess of underlying coverage
Patient Compensation Fund Notes:
- Florida’s standard PCF was dissolved December 31, 2023.
- South Carolina had a PCF; however, effective January 1, 2020, the South Carolina PCF and the South Carolina Medical Malpractice Joint Underwriting Association (JUA) were consolidated into the South Carolina Medical Malpractice Association (SCMMA). As a result, the South Carolina PCF fund is winding down, with the intent for the MMA to evolve into the market of last resort for providers and entities.
Birth Injury Funds
Three states—Florida, New York, and Virginia—have another type of compensation fund focusing on birth-related neurological injuries. These funds and PCFs have elements in common, such as compensation outside the healthcare insurance and malpractice tort system, but function differently than PCFs. Information about the funds here is sourced from the linked websites.
Florida Birth-Related Neurological Injury Compensation Association (NICA)
NICA is a no-fault alternative to medical malpractice litigation. Participating providers are protected from tort action in cases that are accepted into the NICA program. The fund helps “birth-injured children and adults [receive] the care they need while reducing the financial burden on medical providers and families.” A statutory organization, it manages state funds to pay for the lifetime support and care of adults and children born with certain birth-related neurological injuries occurring in a Florida hospital when the obstetrical services were provided by participating providers. Admitted cases are removed from the tort system on a no-fault basis. Families receive an initial lump sum payment and lifetime payments for medically necessary and reasonable expenses for eligible injuries. Provider participation is voluntary for providers practicing in Florida but, generally, all providers are required to inform obstetrical patients of their participation status. Participating physicians and certified nurse midwives (under the supervision of a participating physician) pay an annual assessment. Certain other providers are not required to pay the assessment.
New York Medical Indemnity Fund (MIF)
The New York MIF provides a funding source for certain future healthcare costs of individuals with birth-related neurological injuries as the result of medical malpractice during a delivery admission. Costs are paid throughout the lifetime of an eligible plaintiff after a court-approved settlement or judgment. The fund generally pays for care in excess of health insurance coverage and other programs (except Medicare and Medicaid) but in lieu of the corresponding portion of a court settlement or judgment. Non-domestic providers are eligible for reimbursement of covered expenses under the fund.
Virginia Birth-Related Neurological Injury Compensation Program
For admitted children born with serious birth-related neurological injuries, this fund covers their care including “medically necessary expenses such as medical expenses, hospital expenses, rehabilitation expenses, in-home nursing care” and other costs. Benefits are provided to children with a qualifying birth-injury who were delivered by a participating provider (physician/midwife) or at a participating hospital. Children admitted into the program are not eligible for compensation from a medical malpractice lawsuit. The program is funded without general state funds through fees paid by participating providers and hospitals as well as assessments on liability insurance carriers operating in Virginia and non-participating physicians practicing in Virginia. Except those receiving an exemption, all physicians practicing in Virginia (regardless of specialty) are required to participate in the fund or pay the non-participating assessment and are obligated to inform obstetrical patients of their participation status.
References
- Susan Beach and Eric R. Anderson, “MPL Association—A Rich History of Supporting Insurers and Medical Professionals,” Inside Medical Liability. First Quarter 2022.
- Elizabeth D. Schrero, “Patient Compensation Funds: Legislative Responses to the Medical Malpractice Crisis,” American Journal of Law & Medicine, 1979 Summer;5(2):175-95.

Working with State Funds

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Indiana = $87,349,276
About the same as Colorado ($86,118,826)
Texas is about twice the size ($195,739,891)
Wisconsin is about half the size ($44,158,052)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: $500,000 cap on total damages per provider; $1.8 million cap on total damages for all providers and state fund: UPHELD- Ind. Code Ann. § 34-18-14-3
- Ind. Code Ann. § 34-18-18-1
- Ind. Code Ann. § 34-44-1-2
Statute of limitations: Two years from act or discovery UPHELD
- Ind. Code Ann. § 34-18-7-1
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: At the court’s discretion a simple interest rate of not less than 6% nor more than 10%.- Ind. Code Ann. § 34-51-4-9
- No Prejudgment Interest: Prejudgment interest is not available: a) against the state or any political subdivision, Ind. Code Ann. § 34-51-4-4; b) for claims against the patient’s compensation fund, Ind. Code Ann. § 34-51-4-2; c) on punitive damage awards. Ind. Code Ann. § 34-51-4-3, or d) if the plaintiff or defendant, as applicable, fail to make an offer of settlement as set forth in Ind. Code Ann. § 34-51-4-5 or Ind. Code Ann. § 34-51-4-6.
- Ind. Code Ann. § 24-4.6-1-101
- Ind. Code Ann. § 24-4.6-1-101
Recording Consent
Indiana is a one-party consent state.
In Indiana, it is a criminal offense to use any device to intercept communications, whether wire or electronic, without the consent of at least one person taking part in the communication. Ind. Code Ann. § 35-31.5-2-176. This applies to text messages and e-mails as well. Ind. Code Ann. § 35-31.5-2-110.
Abortion Laws
Indiana enacted a new total ban on abortion, which took effect on August 1, 2023, after the state supreme court vacated the injunction blocking the law.
CME Requirements
CME requirements listed above were updated based on information from the Medical Licensing Board of Indiana, but education requirements do change. Due to COVID-19, certain states may have modified their licensure requirements. Physicians should confirm Indiana’s current requirements provided by the Medical Licensing Board of Indiana.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Pennsylvania = $252,894,722
About the same as Georgia ($281,292,315)
Florida is about twice the size ($543,225,488)
Maryland is about half the size ($126,812,975)
New Business Paper
New MPL policies in the standard market are issued by NORCAL Insurance Company.
Tort Laws
Limits on damages for pain and suffering: None (prohibited by state constitution)Limits on contingent attorney fees: None: Sliding scale ruled unconstitutional
Reform of collateral source rule: Mandatory – bans subrogation
- Stat. Ann. tit. 40, § 1303.508
- Stat. Ann. tit. 40, § 1303.509
- Stat. Ann. tit. 42, § 5524; Pa. Stat. Ann. tit. 40, § 1303.513
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: (Action seeking relief for bodily injury, death or property damage – Delay Damages) Prime rate, as stated in Pa. R.C.P. 238(a)(3). The plaintiff must request delay damages within 10 days of the verdict or decision.- R.C.P. No. 238(a)(3); but see Pa. R.C.P. No. 238(d) (actions heard by a board of arbitrators); 42 Pa. Cons. Stat. Ann. § 8371 (insurance bad faith claims); Touloumes v. E.S.C. Inc., 899 A.2d 343 (Pa. 2006) (prejudgment interest, not delay damages, is recoverable in a breach of contract action where the damages sought are measurable by actual property damage)
- R.C.P. No. 238(a)(2); Pa. R.C.P. No. 238(b)(1)
- Pittsburgh Constr. Co. v. Griffith, 834 A.2d 572 (Pa. Super. Ct. 2003); 41 Pa. Stat. Ann. tit. 41, 202
- 42 Pa. Cons. Stat. Ann. § 8101
Recording Consent
Pennsylvania is a two-party consent state.
In Pennsylvania, it is a criminal offense to use any device to record communications, whether they’re wire, oral or electronic, without the consent of everyone taking part in the conversation. This means that in Pennsylvania you are not legally allowed to record a conversation you are taking part in unless all parties are in agreement. 18 Pa. Cons. Stat. Ann. § 5704.
Abortion Law
Abortion will likely remain accessible in Pennsylvania but without legal protection. The current governor is supportive of abortion rights, but numerous restrictions make it difficult to access abortion care in the state.
CME Requirements
For both MDs and DOs, Pennsylvania requires 100 hours of CME credits per licensure cycle. MDs must complete at least 20 AMA PRA Category 1 Credit™ hours and DOs must complete at least 20 AOA Category 1-A credit hours.
- Physicians renewing their license for the first time are only required to complete 2 hours of board-approved continuing education in child abuse recognition and reporting requirements.
Biennium—beginning Jan. 1 of odd-numbered years through Dec. 31 of even-numbered years for both MDs and DOs.
For the second license renewal and all following renewals, Pennsylvania MDs and DOs must meet the following topical requirements:
- 12 hours of CME focused on patient safety or risk management
- 2 hours of board-approved continuing education in child abuse recognition and reporting requirements
- 2 hours of education pertaining to pain management, the identification of addiction, or in the practices of prescribing or dispensing of opioids (required for all prescribers or dispensers)
The Pennsylvania CME requirements listed above were accurate when posted, but CME state requirements change frequently. Due to COVID-19, certain states may have modified their licensure requirements. Physicians are advised to confirm Pennsylvania’s current requirements with the Pennsylvania State Board of Medicine website and the Pennsylvania State Board of Osteopathic Medicine website.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Wisconsin = $44,158,052
About the same as Arkansas ($45,765,493)
Indiana is about twice the size ($87,349,276)
Idaho is about half the size ($22,723,588)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: $750,000 cap on noneconomic damages. In wrongful death cases, noneconomic damages of $500,000 (for a minor) or $350,000 (for an adult) may be awarded.- Wis. Stat. Ann. §§ 893.55; 895.04
- Wis. Stat. Ann. § 655.013
Periodic payment of future damages: Mandatory (present value of awards over $100,000 go to PCF for distribution)
- Wis. Stat. Ann. § 655.015
- Wis. Stat. Ann. § 893.55
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: For liquidated damages or damages that can be measured to a reasonably certain standard, 5% or amount agreed to, but not to exceed 12%. Prejudgment interest not available where the existence of multiple defendants prevents any single defendant from knowing the precise amount of their liability. If an offer of judgment is made, interest at the rate noted in Wis. Stat. § 807.01(4) may apply.- Wis. Stat. Ann. §§ 138.04, 138.05; Betty Andrews Revocable Trust v. Vrakas/Blum, S.C., 779 N.W.2d 723 (Wis. Ct. App. 2009); Wis. Stat. Ann. § 807.01(4)
- First Wisconsin Trust Co. v. L. Wiemann Co., 286 N.W.2d 360 (Wis. 1980) (contract action – date of breach); Thermal Design, Inc. v. Project Coordinators, Inc., 730 N.W.2d 460 (Wis. Ct. App. 2007) (liquidated damages – date due); Wis. Stat. Ann. § 807.01(4)
- Wis. Stat. Ann. § 814.04(4)
- Wis. Stat. Ann. § 814.04(4)
Recording Consent
Wisconsin is a one-party consent state.
In Wisconsin, it is a criminal offense to use any device to record or share use communications, whether they are wire, oral or electronic, without the consent of at least one person taking part in the communication. This means that in Wisconsin, you are legally allowed to record a conversation if you are a contributor, or with prior consent from one of the involved parties, barring any criminal intentions. Evidence that is obtained by recording communication is 'totally' inadmissible in civil court cases. Regardless of who took the recording, the only way a recording can be admissible in a civil case is with the consent of the person recorded. Wis. Stat. Ann. §§ 968.27; 968.31; 885.365(1).
Abortion Law
Wisconsin legislators seek to prohibit abortion. The current governor is supportive of abortion rights and the Attorney General has sued the Speaker and Majority Leader of the Wisconsin Legislature seeking a declaratory judgment that the pre-Roe ban is unenforceable.
CME Requirements
Physicians must complete 2 credit hours of approved CME in the topic of responsible opioid prescription. Physicians who do not hold a U.S. Drug Enforcement Administration number to prescribe controlled substances are exempt from this requirement. More than 20 CME credits can be earned in any subject area.
The Wisconsin CME requirements listed above were accurate when posted, but CME state requirements change frequently. Due to COVID-19, certain states might have modified their licensure requirements. Physicians are advised to confirm Wisconsin’s current requirements with the Wisconsin Department of Safety and Professional Services.

Texas Legislative Update
The 89th Texas legislative session has come to an end and, happily, the healthcare liability reforms passed in 2003 remain intact. The noneconomic damage caps survived a challenge, persisting at a total of $250,000 for physician defendants and up to two additional $250,000 caps applicable to hospital defendants. The Texas Alliance for Patient Access (TAPA) has kept a close watch on the various bills submitted and has actively lobbied for preservation of the critical medical tort reforms.
Since the reforms passed, and because they have largely remained intact, the rate at which the number of physicians in Texas is growing exceeds that of the general population. As the Chair of TAPA’s Legal and Claims Committee, I am privileged to be among the watchdogs carefully monitoring the legislative landmines healthcare providers could face. Each legislative session presents a challenge. TAPA also considers court cases being appealed, assessing whether and when to file amicus curiae, or “friend of the court” briefs, to provide additional perspective, information, and expertise to the reviewing courts. Visit TAPA.info for more information.
Brian Jackson, Executive Director, Texas Alliance for Patient Access (TAPA) created this non-exhaustive summary of bills that were proposed and defeated this session:
This bill sought to remove vicarious liability for nonprofit health organizations that employ physicians. The bill failed to pass, but the Texas Supreme Court recently issued the Renaissance Medical Foundation v. Lugo* opinion, which addresses most of the issues set forth in the bill.
Also defeated were proposed noneconomic damage caps that would apply to personal injury claims other than medical malpractice. Our concerns about those proposals were that they proposed far higher caps on noneconomic damages (one at $1 million, another at $5 million). We feared that if these caps were passed, the medical malpractice noneconomic damage cap would pale in comparison and be far more difficult to maintain at current levels.
About Texas Alliance for Patient Access (TAPA)
The Texas Alliance for Patient Access is a statewide coalition of doctors, clinics and hospitals, nursing homes, and professional liability insurers that was formed in 2001, a time when many professional liability insurers could not afford to remain in the state. TAPA’s mission was to improve access to care by relieving the stresses on providers and insurers through meaningful medical liability tort reform. It successfully lobbied for comprehensive legislation passed in 2003, which included a statutory cap on noneconomic damages and was followed by constitutional amendment approved by Texas voters. Other reforms included limitation of evidence of medical expenses to those actually paid or incurred (as opposed to billed), periodic payment of future damages, expert witness requirements, a heightened burden of proof applicable to emergency care, and a restatement of the wrongful death damage cap.
---
* See Renaissance Medical Foundation v. Lugo, 2025 WL 178694, 68 Tex. Sup. Ct. J. 951 (Tex. 2025) (recognizing applicable statute eliminates vicarious liability claims against nonprofit health organizations that are based upon a physician’s negligent exercise of independent medical judgment).


Securing Large Markets

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
California = $459,025,180
About the same as Florida ($543,225,488)
New York is about twice the size ($833,107,315)
Pennsylvania is about half the size ($252,894,722)
New Business Paper
New MPL policies in the standard market are issued by NORCAL Insurance Company.
Tort Laws
Limits on damages for pain and suffering: $430,000 tiered noneconomic cap (all physicians/up to two separate institutions) for personal injury, increases $40k/year through 2033; $600,000 tiered noneconomic cap for wrongful death, increases $50k/year through 2033). Annual 2% increase after 2033.- Civ. Code Ann. § 3333.2
- Bus. & Prof. Code Ann. § 6146
- Civ. Code Ann. § 3333.1
- Civ. Proc. Code Ann. § 667.7
- Civ. Proc. Code Ann. § 340.5
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate:- General Rule: 7%
- Const. Art. XV, § 1
- Personal Injury Tort Actions Where Offer to Compromise Was Made: Except for actions against public entities and their employees, if a plaintiff in a personal injury action makes an offer of compromise that is rejected, a plaintiff is entitled to interest at a rate of 10% per year if the judgment is greater than the offer of compromise.
- Cal. Civ. Code Ann. § 3291
- General Rule: If ascertainable, from the date ascertainable. Otherwise, at the discretion of the jury.
- Levy-Zentner Co. v. S. Pac. Transp. Co., 142 Cal. Rptr. 1 (Cal. Ct. App. 1977) (property damage case); Cal. Civ. Code Ann. §§ 3287; 3288
- Personal Injury Tort Actions Where Offer to Compromise Was Made: Date of the offer of compromise.
- Cal. Civ. Code Ann. § 3291
- Civ. Proc. Code Ann. § 685.010
- Civ. Proc. Code Ann. § 685.020(a); but see Cal. Civ. Code Ann. § 685.020(b) (installment payments)
Recording Consent
California is a two-party state.
In California, it is a criminal offense to use any device to record communications, whether they’re wire, oral, or electronic, without the consent of everyone taking part in the communication. This means that in California you are not legally allowed to record a conversation you are taking part in unless all parties are in agreement. However, an exception applies if the conversation takes place in public, within government proceedings open to the public, or under conditions where one could reasonably expect to be overheard. Cal. Penal Code Ann. § 632
Abortion Law
Abortion will remain legal in California. The state’s highest court recognized abortion rights under the California Constitution in 1969, four years before Roe. State law protects the right to personal reproductive decisions. In November 2022, Californians approved Prop 1, which explicitly adds abortion and contraception rights to the state constitution.
CME Requirements
- For MDs, California requires 50 hours of approved CME credits per licensure cycle. All must be Category 1 approved.
- For DOs, licensees must complete a total of 100 credit hours per licensure cycle (50 credits each year); 20 hours must be AOA Category 1A or 1B.
Physicians (with exemptions for radiologists and pathologists) must complete a one-time CME course in pain management and the treatment of terminally ill and dying patients. There are two ways to meet these requirements.
- By completing 12 CME hours in the treatment and management of patient with opioid use disorders. If this course is chosen it must include 8 hrs. of CME in buprenorphine treatment or other opioid replacement therapy.
OR - Physicians may complete 12 hours of pain management and/or the treatment of patients who are terminally ill/at the end of life. Any combination of courses in these topic areas are acceptable.
CME requirements listed above were updated based on the Medical Board of California's information, but education requirements do change. Certain states might have modified their licensure requirements due to COVID-19. Physicians should confirm California's current requirements on the Medical Board of California's Continuing Medical Education page.

- Physician Market Comparison
- New Business Paper
- Department of Insurance Reporting
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Florida = $543,225,488
About the same as California ($459,025,180)
Georgia is about half the size ($281,292,315)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Department of Insurance Reporting
The Florida Department of Insurance publishes an annual report outlining market trends, examinations and investigations, insurance regulations, and more. A section on the state of property and casualty is included. The most recent report currently available is from 2022.
Tort Laws
Limits on damages for pain and suffering: None- Fla. Stat. Ann. § 766.118 Ruled unconstitutional by State Supreme Court (June 2017)
- Fla. Const. art. I, § 26
- Fla. Stat. Ann. § 768.76
- Fla. Stat. Ann. § 768.78
- Fla. Stat. Ann. § 95.11
Prejudgment and Post-Judgment Interest
Prejudgment interest rates only apply to contract actions.
Prejudgment Tort Actions Rate: The rate of interest established in the contract, if any. If no rate is established, the rate established by the State’s Chief Financial Officer.- Fla. Stat. Ann. § 687.01; Fla. Stat. Ann. § 55.03
- Argonaut Ins. Co. v. May Plumbing Co., 474 So.2d 212 (FL 1985)
- Fla. Stat. Ann. § 55.03
- Fla. Stat. Ann. § 55.03; Amerace Corp. v. Stallings, 823 So.2d 110 (FL 2002)
Recording Consent
Florida is a two-party state.
In Florida, it is a criminal offense to use any device to record communications, whether wire, oral, or electronic, without the consent of everyone taking part in the communication. This means that in Florida you are not legally allowed to record a conversation you are taking part in unless all parties are in agreement. Fla. Stat. Ann. § 934.03(2)(d)
Abortion Law
Florida is enforcing a six-week ban.
CME Requirements
- Group 1 licenses expire in years ending in even numbers.
- Group 2 licenses expire in years ending in odd numbers.
For MDs:
- Second and subsequent renewals require 40 hours including two hours of Category 1 or 2 on prevention of medical errors.
- Every third renewal requires 40 hours, including two hours of Category 1 or 2 in prevention of medical errors and two hours of Category 1 or 2 in domestic violence.
- Each person registered with the DEA and authorized to prescribe controlled substances must complete two hours of AMA Category 1 or AOA Category 1-A on prescribing controlled substances for each biennial renewal.
For DOs:
- Beginning in the 2010-2012 licensure biennium, five of the CME hours must include one hour in each of the following topics: (1) professional and medical ethics education, (2) Florida laws and rules, and (3) federal and state laws related to the prescribing of controlled substances; and two hours required in the Prevention of Medical Errors.
- Every third biennial renewal, licensee shall complete a two-hour domestic violence course.
- Licensee must complete a one-hour HIV/AIDS course no later than upon the first biennial renewal.
- Twenty hours of general, AOA Category 1-A CE related to the practice of osteopathic medicine or under osteopathic auspices.
The Florida CME requirements listed above were accurate when posted, but CME state requirements change frequently. Due to COVID-19, certain states may have modified their licensure requirements. Physicians are advised to confirm Florida’s current requirements with the Florida Board of Medicine.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Maryland = $126,812,975About the same as Tennessee ($127,225,243)
Pennsylvania is about twice the size ($252,894,722)
Oklahoma is about half the size ($64,608,595)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: $950k cap on non-economic damages with $15k annual increase- Md. Code Ann. Cts. & Jud. Proc. § 3- 2A-09
- Md. Code Ann. Cts. & Jud. Proc. § 3-2A-07
Periodic payment of future damages: Discretionary
- Md. Code Ann. Cts. & Jud. Proc. § 11-109
- Md. Code Ann. Cts. & Jud. Proc. § 5-109
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: Generally, because damages are unliquidated, interest is not allowed.- Taylor v. Wahby, 314 A.2d 100 (MD 1974)
- Md. Code Ann. Cts. & Jud. Proc. § 11-107
- Md. Rules 2-604
Recording Consent
Maryland’s Wiretapping and Electronic Surveillance Act stipulates that it is a two-party state. In this state, it is a criminal offense to tape-record a conversation without the consent of all involved parties. Md. Code Ann. Cts. & Jud. Proc. § 10-402
Abortion Law
Abortion remains legal in Maryland. In 2024, voters decided to amend the Maryland Constitution to create a right to reproductive freedom.
CME Requirements
Maryland requires 50 hours of Category 1 CME credits per licensure cycle. First-time license renewals are exempt from CME requirements.
A required one hour must be on opioid prescribing.
The Maryland CME requirements listed above were accurate when posted, but CME state requirements change frequently. Due to COVID-19, certain states may have modified their licensure requirements. Physicians are advised to confirm Maryland’s current requirements with the Maryland Board of Physicians.

Eyes on Legislation in Key States
We are monitoring legislative and legal decisions across the country and their impacts on the medical professional liability space.
Title: An Act to Establish Recovery of Damages for Necessary Medical Care, Treatment, or Services Rendered; and for Other Purposes
Last Action: Notice that HB 1204 is now Act 28
Summary: The legislation states that past medical damages may not exceed the amount actually paid or unpaid amounts for which the claimant—or other third party—is legally responsible.
Title: An Act to Amend the Law Concerning Miscellaneous Prohibited Practices Under the Arkansas Insurance Code; to Clarify Fees Collected by Certain Brokers; and for Other Purposes
Last Action: Notice that SB 76 is now Act 23
Summary: It allows surplus lines brokers to charge certain fees and waives limits on those fees if a risk is referred to them by a P&C agent or broker.
Title: An Act to Amend the Law Concerning Standards for Insurance Policies; to Revise the Notice Requirements of an Insurer for a Premium Increase; and for Other Purposes
Last Action: Notice that SB 70 is now Act 22
Summary: This act requires insurers to provide a notice of at least 60 days of any premium increase equal to or greater than 25%.
Title: Georgia Courts Access and Consumer Protection Act
Last Action: The act will go into effect January 1, 2026.
Summary: This new legislation requires litigation financers to completely disclose terms and conditions of contracts to consumers. It also prohibits commissions from referring consumers to litigation funders or from litigation funders to specific law firms or healthcare providers. It makes such funding arrangements discoverable but not admissible.
Title: Civil Practice; Substantive and Comprehensive Revision of Provisions Regarding Civil Practice, Evidentiary Matters, Damages, and Liability in Tort Actions
Last Action: This act went into effect April 21, 2025.
Summary: This act prevents references to specific noneconomic damages amounts during the negligence phase of a trial, except during opening and closing arguments. It only allows the reference during the closing arguments if it was brought up during the opening. These references must be the same dollar value. It also allows evidence of both amounts billed and amounts actually paid.
Title: Limiting Discovery and Disclosure of Third-Party Litigation Funding Agreements and Requiring Reporting of Such Agreements to Courts
Last Action: It was approved by the governor on April 7, 2025.
Summary: This legislation establishes disclosure requirements for third-party litigation funding agreements. It also limits the definition of these kinds of agreements to ones where funds are used to directly support litigation.
Title: Enacting the Help Not Harm Act, Restricting Use of State Funds to Promote Gender Transitioning, Prohibiting Healthcare Providers from Providing Gender Transition Care to Children …
Last Action: Governor’s veto was overridden on February 18, 2025.
Summary: This legislation states that medical professional liability insurance policies will not cover damages for healthcare providers who provide gender-affirming care for minors.
Title: An Act Relating to Consumer Data Privacy
Last Action: This was signed by the governor on March 15, 2025.
Summary: The new legislation exempts from the state’s consumer privacy law any information collected by a healthcare provider that maintains protected health information in accordance with HIPAA.
Title: An Act to Amend and Reenact Civil Code… Relative to Comparative Fault; to Establish a Modified Comparative Fault System; to Provide for the Recovery of Damages …
Last Action: It was signed by the governor on May 28, 2025, and became Act 15.
Summary: The legislation requires damages to be assessed based on the percentage of fault attributed to the defendant. If the plaintiff is 51% or more at fault, no damages will be awarded.
Title: Provide Immunity from Liability for Cybersecurity Events
Last Action: The bill was approved by the governor on March 17, 2025.
Summary: This legislation protects private entities from class action lawsuits resulting from a cybersecurity event except when those entities cause the breach through willful, wanton, or gross negligence.
Title: An Act Relating to Civil Actions; Revising Provisions Relating to Alternative Dispute Resolution for Certain Civil Actions; and Providing Other Matters Properly Relating Thereto
Last Action: This bill was approved by the governor on June 3, 2025.
Summary: This bill increases the threshold for mandatory, nonbinding arbitration from $50,000 to $100,000. It also removes limitations on arbitrator compensation requires that fees and costs be established by rules.
Title: An Act Relating to a Limitation of Civil Liability of Business Entities in Connection with a Breach of System Security
Last Action: This bill was sent to the governor on June 1, 2025.
Summary: This bill would create a safe harbor against punitive damages in cybersecurity breach lawsuits for small businesses that maintain reasonable cybersecurity programs. A cybersecurity program may meet the requirements of the law if it conforms to various industry standards and complies with applicable laws, including HIPAA and HITECH.
Title: Medical Malpractice Modifications
Last Action: This was signed by the governor on March 27, 2025.
Summary: This act states damages may not be considered until a finding of fault is rendered, and economic damages for medical costs can only include amounts actually paid by the patient or insurer. It also establishes steps for pre-litigation review panels and requires data from the panels to be reported to the state.
Title: Punitive Damages Amendments
Last Action: The governor signed this bill on March 25, 2025.
Summary: Stipulates that punitive damages over $50,000 do not have to be split between the plaintiff and the state after May 11, 2025.
Title: Nursing Homes and Certified Nursing Facilities; Professional Liability Insurance, Proof of Coverage
Last Action: The legislation was approved by the governor on March 21, 2025.
Summary: This increases the liability coverage nursing homes and skilled nursing facilities must carry to $1M in noneroding general liability coverage per occurrence and medical liability coverage up to the full amount of the damage cap—the damage cap is currently $2.65M—per patient occurrence.

Establishing a National Footprint
Like many MPL carriers that grew out of the med-mal crisis in the 1970s, ProAssurance has achieved significant growth through mergers and acquisitions. These transactions allowed the company to gain significant presence in key areas around the state—allowing ProAssurance to both invest in expertise in local markets as well as establish a nationwide footprint.
Physicians Insurance Company of Michigan (PICOM) was formed in1980 to assume the Brown-McNeely Fund’s business, a state fund created to address the dearth of affordable professional liability coverage. PICOM would continue to grow to become Professionals Group, which merged with Medical Assurance to form ProAssurance in 2001.
MAIC Holdings (later Medical Assurance) acquired Missouri Medical Insurance Company (MOMEDICO), a publicly traded insurer, in 1998—expanding westward and providing a base for operations in the Central U.S. Medical Assurance also assumed the business of Medical Defense Associates to strengthen its commitment to the state of Missouri in 1999.
PICOM assumed the business of Physicians Insurance Company of Ohio (PICO) in 1995, a starting point of operations for Midwest expansion. ProAssurance also purchased renewal rights to Ohio Hospital Insurance Company’s physician, hospital, and healthcare facility business in 2004.
ProAssurance acquired NCRIC Group, Inc. in 2005, a parent company of NCRIC, Inc. (an insurer serving Washington, D.C. and Mid-Atlantic states), including Virginia and Washington D.C.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Michigan = $151,134,721About the same as Virginia ($139,417,623)
Georgia is about twice the size ($281,292,315)
Connecticut is about half the size ($73,203,697)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: $586,300 cap on non-economic damages with exceptions reaching $1,047,000 (all amounts adjusted for inflation on 12/31)- Mich. Comp. Laws Ann. § 600.1483
- MI R ADMIN MCR 8.121(B)
- Mich. Comp. Laws Ann. § 600.6303
- Mich. Comp. Laws Ann. § 600.6307
- Mich. Comp. Laws Ann. §§ 600.5805; 600.5838a
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: 1% above the average interest rate paid at auctions of 5-year U.S. treasury notes during the 6 months immediately preceding July 1 and January 1, compounded annually. Rate calculated at 6-month intervals. Interest is calculated on the entire money judgment, including attorney fees and other costs (Complaints filed on or after Jan. 1, 1987).- Mich. Comp. Laws Ann. § 600.6013(8)
- Mich. Comp. Laws Ann. § 600.6013(8)
- Mich. Comp. Laws Ann. § 600.6013(7), (8)
Recording Consent
Michigan is a two-party consent state.
It is a criminal offense to use any device to record, obtain, use or share communications, whether they're wire, oral or electronic, without the consent of all contributing parties. This means that in Michigan you are not legally allowed to record a conversation you are taking part in unless all parties are in agreement.
However, one court has interpreted that Michigan’s eavesdropping law only applies to third parties and decided it was legal for a contributing party to record a conversation without the other parties’ permission. Sullivan v. Gray, 324 N.W.2d 58 (Mich. Ct. App. 1982).
Abortion Law
Michiganders have approved Prop 3, which enshrines reproductive freedom in the Michigan constitution.
CME Requirements
For both MDs and DOs, Michigan requires 150 hours of CME credits of courses or programs approved by the board, per licensure cycle. No one, including medical school faculty and resident physicians, is exempt from this requirement.
For MDs 75 CME hours must be Category 1 while for DOs 60 hours must be Category 1. A minimum of 1 hour of continuing education must be earned in the area of medical ethics. The majority of CME credits can be taken on any topic area. Effective December 6, 2017, a minimum of 3 hours of continuing education must be earned in the area of pain and symptom management.
- Human Trafficking Training – Beginning December 6, 2021, completion of a one-time training to identify victims of human trafficking is required for individuals seeking licensure that meets the standards of Administrative Rule 338.2413.
- Implicit Bias Training – Beginning June 1, 2022, completion of 2 hours of implicit bias training within the 5 years immediately preceding issuance of the license or registration is required.
The Michigan state CME requirements listed above were accurate when posted. CME state requirements change frequently. Certain states might have modified their licensure requirements due to COVID-19. Physicians are advised to confirm requirements with the Michigan Board of Medicine.

- Physician Market Comparison
- New Business Paper
- Department of Insurance Reporting
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Missouri = $92,424,043About the same as Alabama ($93,744,311)
Texas is about twice the size ($195,739,891)
Kansas is about half the size ($45,902,496)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Department of Insurance Reporting
The Missouri Department of Insurance publishes a variety of annual reports, including a Medical Professional Liability Insurance Report and Market Share Report.
Tort Laws
Limits on damages for pain and suffering: $473,445 cap on non-economic damages with exceptions reaching $828,529 for catastrophic injury or death (amounts adjusted by 1.7% annually on 1/1)- Mo. Rev. Stat. Ann. § 538.210
Reform of collateral source rule: None
Periodic payment of future damages: Mandatory over $100k at request of either party
- Mo. Rev. Stat. Ann. § 538.220
- Mo. Rev. Stat. Ann. § 516.105
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: If the claimant has made a demand for payment or an offer of settlement and the amount of the judgment exceeds the demand for payment or offer of settlement, the Federal Funds Rate (established by the Federal Reserve) plus 3%.- Mo. Rev. Stat. Ann. § 408.040(3), (4)
- Mo. Rev. Stat. Ann. § 408.040(3)
- Mo. Rev. Stat. Ann. § 408.040(3)
- Mo. Rev. Stat. Ann. § 408.040(3)
Recording Consent
Missouri is a one-party state.
It is a criminal offense to use any device to record or share communications, whether wire or oral, without the consent of at least one contributing party. This means that in Missouri you are not legally allowed to record a wire or oral conversation you are taking part in unless you have the consent of at least one party. Mo. Rev. Stat. Ann. § 542.402(2)(3)
This state does stipulate that electronic communications can be lawfully recorded or shared with the consent of at least one party, barring any criminal intentions. This applies to conversations where all contributing parties are using a cell phone, including text messages sent between cell phones. However, a Missouri appellate court determined that a conversation taking place where one party is using a cell phone and the other is using a regular wire phone is indeed protected under the wiretap law. Lee v. Lee, 967 S.W.2d 82 (MO Ct. App. 1998)
Abortion Law
Voters approved a 2024 amendment to the Missouri Constitution to protect reproductive freedom. A state circuit court held that the state’s trigger ban and other abortion restrictions were enjoined as unconstitutional; however, on May 27, 2025, the Missouri Supreme Court temporarily blocked those injunctions allowing the trigger ban to go into effect.
CME Requirements
Missouri physicians are required to complete 50 hours of AMA PRA Category 1 Credit™ or AOA Category 1-A CME per licensure cycle.
As of February 2021, the Missouri Division of Professional Registration does not have specific requirements. It allows physicians to self-select topics around which they can earn CME and meet licensure requirements.
CME requirements listed above were updated based on information from the Missouri Division of Professional Registration, but education requirements do change. Due to COVID-19, certain states may have modified their licensure requirements. Physicians should confirm Missouri's current requirements on the Missouri Division of Professional Registration’s Healing Arts page.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Ohio = $113,469,930
About the same as Maryland ($126,812,975)
Pennsylvania is about twice the size ($252,894,722)
South Carolina is about half the size ($58,554,971)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: Greater of $250k or three times economic damages up to max of $350k/plaintiff, $500k/occurrence ($500k/plaintiff and $1 million/occurrence in catastrophic cases)- Ohio Rev. Code Ann. § 2323.43
- Ohio Rev. Code Ann. § 2323.43(F)
- Ohio Rev. Code Ann. § 2323.41
- Ohio Rev. Code Ann. § 2323.55
- Ohio Rev. Code Ann. § 2305.113
Prejudgment and Post-Judgment Interest
Prejudgment interest is allowed on judgments rendered against the state for the same time period and rate as allowed between private parties. The court may exercise its discretion to deny interest for periods of undue delay after commencement of the action. However, no interest is allowed on settlements. Ohio Rev. Code Ann. §§ 2743.18(A); 2743.15(B)
Prejudgment Tort Actions Rate: If prejudgment interest is allowed because the parties failed to make a good faith effort to settle the case, the rate is the federal short-term rate plus 3%.- Ohio Rev. Code Ann. §§ 5703.47; 1343.03(A); 1343.03(C)
Post-Judgment Tort Actions Rate: Unless a contract requires otherwise, the federal short-term rate plus 3%.
- Ohio Rev. Code Ann. §§ 1343.02; 5703.47; 1343.03(B)
- Ohio Rev. Code Ann. § 1343.03(B)
Recording Consent
Ohio is a one-party state.
In Ohio, In Ohio, it is a criminal offense to use any device to record or share communications, whether wire, oral, or electronic, without the consent of at least one person taking part in the communication. This means that in Ohio, you are legally allowed to record a conversation if you are a contributor, or with prior consent from one of the involved parties, barring any criminal intentions. Ohio Rev. Code Ann. § 2933.52.
Abortion Law
Ohioans have approved a constitutional amendment that protects reproductive decision making. The state’s six-week ban has been permanently blocked.
CME Requirements
Ohio requires 50 hours of CME credits per licensure cycle. For first-time renewal, a licensee’s required hours will be prorated based on the number of months for which the individual has been licensed. Physicians renewing their license must complete 50 hours of CME designated by the AMA as AMA PRA Category 1 Credit™, by the AOA as category 1-A or 2-A, or by the APMA as category 1. Physicians residing or practicing outside of Ohio, and physicians who are not currently practicing, must complete CME requirements if they wish to maintain their license. Reinstatement CME requires the above criteria within 24 months prior to submission and must be completed before reinstating a license.
As of May 2021, physicians are required to complete one hour of CME on the topic of a licensee’s duty to report misconduct to the State Medical Board of Ohio. The remaining CME hours do not have specific topical requirements.
The Ohio CME requirements listed above were accurate when posted, but CME state requirements change frequently. Due to COVID-19, certain states may have modified their licensure requirements. Physicians are advised to confirm Ohio’s current requirements with the State Medical Board of Ohio.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Virginia = $139,417,623About the same as Arizona ($135,063,401)
Georgia is about twice the size ($281,292,315)
Nevada is about half the size ($69,084,099)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: $2.65 million cap on total damages (annual increases of $50,000 from 7/1/2012 through 7/1/2031)- Code Ann. § 8.01-581.15
Reform of collateral source rule: None
Periodic payment of future damages: Discretionary (at court option - no statutory citation)
Statute of limitations: Two years; 10-year maximum; one-year Foreign Object exception
- Code Ann. § 8.01-243
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: 6%, or amount provided in contract, if higher. However, the award of interest is discretionary.- Code Ann. §§ 8.01-382; 6.2-302; Dairyland Ins. Co. v. Douthat, 449 S.E.2d 799 (Va. 1994)
- Upper Occoquan Sewage Auth. v. Blake Constr. Co., 655 S.E.2d 10 (Va. 2008)
- Code Ann. §§ 8.01-382; 6.2-302
- Code Ann. § 8.01-382; Upper Occoquan Sewage Auth.
Recording Consent
Virginia is a one-party consent state.
In Virginia, it is a criminal offense to use any device to record or share use communications, whether they are wire, oral or electronic, without the consent of at least one person taking part in the communication. This means that in Virginia, you are legally allowed to record a conversation if you are a contributor, or with prior consent from one of the involved parties. Va. Code Ann. §§ 19.2-61, 19.2-62.
Abortion Law
Abortion will remain accessible in Virginia, but without legal protection. In 2020, Virginia repealed numerous restrictions on abortion access.
CME Requirements
Virginia requires 60 CME course hours per licensure period. There are no requirements for first time renewals.
Biennial and expires on the last day of the licensee's birth month.
All 60 CME hours may be type 1 hours, no more than 30 type 2 hours are allowed. Licensees regardless of specialty must complete 2 hours of a type 1 controlled substance course. Roughly 50 CME credits can be taken on any topic area.
The Virginia CME requirements listed above were accurate when posted. CME state requirements change frequently. Certain states might have modified their licensure requirements due to COVID-19. Physicians are advised to confirm Virginia’s current requirements with Virginia’s Board of Medicine.

- Physician Market Comparison
- New Business Paper
- Tort Laws
- Prejudgment and Post-Judgment Interest
- Recording Consent
- Abortion Law
Physician Market Comparison
Washington, D.C. = $15,424,035
About the same as Rhode Island ($14,766,306)
Delaware is almost twice the size ($25,493,816)
Vermont is about half the size ($7,432,531)
New Business Paper
New MPL policies in the standard market are issued by ProAssurance Indemnity Company, Inc.
Tort Laws
Limits on damages for pain and suffering: None
Limits on contingent attorney fees: None
Reform of collateral source rule: None
Periodic payment of future damages: None
Statute of limitations: Three years from discovery
- D.C. Code Ann. § 12-301
Prejudgment and Post-Judgment Interest
Prejudgment Tort Actions Rate: Prejudgment interest is neither authorized nor forbidden by statute. However, a court may award interest, in its discretion, if needed to make the plaintiff whole.- Duggan v. Keto, 554 A.2d 1126 (DC 1989); Burke v. Groover, Christie & Merritt, P.C., 26 A.3d 292 (DC 2011)
- D.C. Code Ann. § 28-3302
- D.C. Code Ann. § 15-109; Bell v. Westinghouse Elec. Co., 507 A.2d 548 (DC 1986)
Recording Consent
Washington, D.C., is a one-party state.
In Washington, D.C., it is a criminal offense to use any device to record communications whether wire, oral, or electronic, without the consent of at least one person taking part in the communication. There is a caveat in that recording is allowed to take place if there is no reasonable expectation of privacy, such as a public place such as a street or park. It should also be noted that the law is applied differently on recordings of audio, video, and audio with video. D.C. Code Ann. § 23-542
Abortion Law
Abortion is protected in Washington, D.C.
CME Requirements
Washington, D.C., requires 50 hours of CME credits per license renewal cycle. First-time license renewals have no CME requirements.
- As part of the 2018 renewal process, physicians, physician assistants, and nurses must complete three hours in the subject of HIV/AIDS, two hours in the subject of LGBTQ cultural competency, and at least one course in the subject of pharmacology.
Washington, D.C., CME requirements listed above were accurate when posted, but CME requirements change frequently. Due to COVID-19, certain licensure requirements may have been modified. Physicians are advised to confirm the District’s current requirements with the District of Columbia Board of Medicine.

Tennessee Supreme Court Finds Quality Improvement Committee Privilege Can Be Waived
Payton Castillo v. David Lloyd Rex, MD, et al.
Summary: The Tennessee Supreme Court found that the quality improvement committee (QIC) privilege provided under Tennessee Code Annotated section 68-11-272 can be waived regarding Payton Castillo v. David Lloyd Rex, MD, et al. The case potentially impacts precedent regarding all medical professional liability cases.
The lawsuit was brought by the wife of a deceased plaintiff against several healthcare providers and organizations who were involved in his care. Those defendants included CHI Memorial Hospital, who formed a QIC to evaluate the quality of care that was given to Mr. Castillo. When the hospital’s representatives explained the circumstances of care with the plaintiff’s widow, they shared protected QIC information with her. The plaintiff’s widow then attempted to discover the statements; however, Memorial claimed they were privileged and undiscoverable.
The trial court and Court of Appeals in Tennessee found this information was discoverable, and the courts concluded the meeting was separate from a QIC proceeding and privilege did not apply. They stated that the information disclosed falls within the protections of the QIC statute and that the privilege belonged to Memorial; however, Memorial waived its privilege when the chief operating officer voluntarily shared the information.
ProAssurance Southeast Regional Risk Manager Bradley Byrne weighed in on the recent ruling:
“The Castillo ruling makes it clear: If providers or hospitals share conclusions from a quality improvement review during a patient disclosure, they risk waiving legal privilege. This decision highlights the importance of structuring disclosure conversations carefully, balancing transparency with the need to protect sensitive internal findings. Providers should work closely with risk management or legal counsel to ensure privilege isn’t inadvertently waived during these critical conversations.”

Getting to Know the ProAssurance Actuary Team
As we take a look at our key states, we also want to bring a spotlight to our Actuarial Team, which supports all of MPL and plays a collaborative and interconnected role across other areas of ProAssurance.
We talked to team members and got some insight into the department. They told us what they do—and what they don’t do—and shared some of the challenges and rewards inherent in their respective positions.








The Actuarial department has many functions, but they all revolve around two primary objectives: rates and reserves. We also do a little bit of reporting on key operational metrics.
– Sokol Berisha, Chief Actuary Officer (5 years with the Actuary team)
[We are] responsible for ratemaking, reserving, large account pricing, data science initiatives, and operational reporting and analysis that support both actuarial and underwriting functions.
– Adalene Woodroof, Manager of Actuarial Underwriting Analysis (5 years, 12 total with ProAssurance)
Projects future costs for policies not yet written so that we can prepare rate filings for the rates in the Underwriting manuals and assist in the pricing of large accounts.
– Glenn Stewart, Director of Actuarial Services (21 years in July)
We handle project needs to maintain company solvency and set a policyholder rating that is reasonable and not unfairly discriminatory.
– Bruce Williams, Assistant Vice President of Actuarial Services (21 years)
“Rates are the dollars we charge to take on future liabilities,” Sokol explains. “This function can be done at a state level, meaning in the state of Alabama this is what we will charge a family physician, or it can be done at an account level where you incorporate the experience of that account. Generally, accounts that are larger will be individually priced … Reserves, on the other hand, are when the company writes a policy, we need to put aside money to pay for future losses. As an insurance company, the biggest liability on our balance sheet is the future losses we will have to pay for policies we have sold … At the end of the day, we sell a promise that we will be there when you need us. Having enough money in the bank to fulfill that promise is paramount.”
In 2022, the Actuarial department established a data science unit to help evaluate risk. “The primary goal of this unit," says Sokol, “is to enhance our ability to differentiate risks at the individual provider level.” Using innovative tools and technology with predictive modeling, the team is able to assist Underwriting in risk selection and in proper pricing. “We are pushing the boundaries of what is possible in the MPL space,” he adds.
The team will prepare data for an external analysis, and that data goes through internal analysis for purposes of projecting future costs of claims for policies that have already been written. With this new information, Glenn explains, “the company can determine the necessary reserves we need to pay our future claim liabilities” (an aggregate adjustment applied to an aggregation of individual claims reserves which are determined by the Claims department).
The team also prepares quarterly and annual financial reporting for certain exhibits.
We asked team members, what are some of your duties?
Sokol: Talking! Most of my time is spent meeting with various leaders in my team to ensure we are making progress on our priorities. Or I am meeting with outside groups to discuss various other initiatives that we are working on collectively!
My job duties at this level are primarily to ensure that my team has the resources required to fulfill and exceed their objectives. I am there to help ensure that our department objectives are aligned with our strategic initiatives and to help each member achieve the goals we set at the beginning of the year.
The biggest item that is fully my responsibility is that each quarter I meet with senior management to make recommendations on the financial performance of ProAssurance. Based on my recommendations, which of course are based on the hard work of my entire team, management will book both current and prior accident years’ reserves. This number is what drives our operating ratios each quarter.
Tonya Bussey (Vice President of Actuarial Services - 24 years): Working with my team to determine the appropriate medical professional liability rate levels to charge for our various programs.
Bruce: Projecting ultimate aggregate claim payouts for liabilities already incurred for which the company is liable and projecting prices needed by customer for liabilities we are incurring as we write new policies. We tailor those prices to the exposure represented by the specific policyholder.
Glenn: I am primarily involved with the reserving and reporting side, as mentioned above. This means making sure we get the data together and we prepare the necessary information for management to make reserving decisions, as well as making sure we complete the reporting we are responsible for on time.
Ted Pyle (Director of Actuarial Services - started with NORCAL in 2002): Primarily large account pricing.
Adalene: I am responsible for calculating and analyzing key monthly metrics, compiling quarterly reports for executive leaders and regional leadership, developing tools to support book-of-business management and profitability analysis, and collaborating cross-functionally to address business needs through tailored ad hoc reporting.
Kenneth Saunders (Senior Actuarial Analyst - 15 years): Preparing reserve schedules (Schedule P, etc.) and loss report controls/maintenance.
Jean-Paul Kapuya (Actuarial Analyst - 20 years): Developing and analyzing rate indications and loss development factors and selecting trend rates. I prepare rate analyses for rate-making decisions. On top of those duties, I also perform class plan and territory analysis for most rate reviews when historical data is available.
Finally, I enjoy representing Actuarial in company functions and work cooperatively with other teams on projects and in meetings. (I currently serve as the chairperson of the Birmingham office wellness committee.)
Sokol: My favorite part of being an actuary is how interconnected we are with various departments within the organization. For example, I work very closely with the Claims team to ensure that we are correctly interpreting the trends we are seeing in the loss data, whether that is claim close ratios or average case reserves that they are setting up in individual states.
We work with Underwriting to ensure we are appropriately charging risks for the potential exposure they represent to the company. This is at the state level but also at each individual account.
We also work with Business Development and Marketing to ensure we release new products that will make us competitive in a particular state.
Working in Actuarial, I really feel like I get to interact with each part of ProAssurance. That is gratifying to me as it helps you understand the whole picture.
Tonya: Numbers, numbers, numbers! I have always enjoyed being able to connect mathematics to the real world; working in insurance was the ideal choice for being able to connect the two.
On the pricing side, we get to analyze claims and exposure data to determine which risks are more likely to have claims, and how big the claims are likely to be. Since we work in the medical professional liability space, we usually only have tens of thousands of records in our sandbox to work with (compared to actuaries working in auto and homeowners who usually have tens of millions of records in their data sets). With a relatively small data set, we frequently need to reach out to our business partners in Underwriting, Business Development, Claims, Risk Management, and elsewhere to help us connect the dots between the trends that we discover in the numbers and the real-world causal factors. The actuary can identify the spike in claims severity. It takes input from our team members in Claims and elsewhere to help us understand the “why” behind the spike.
Bruce: Finding new ways to address the everchanging landscape impacting our projections of the future.
Glenn: One thing I enjoy is the challenge of basically attempting to predict the future for this long-tail line of business. The nature of the MPL line means that the payments you are projecting now will be made over many years into the future. This adds an extra layer of challenge, but I believe it makes it more interesting than perhaps some quicker-paying lines of business. Just the whole concept that, unlike a factory where you just add up the costs of part A, B, and C that make up product D (which is certain because you can look at the receipts), we sell a product where we literally don’t know what it costs yet. Ultimately, we have to wait to find out if we were correct, but we still have to figure out a price to charge today. I just find it fascinating.
Ted: Collaborating with other teams to develop optimal solutions for our largest accounts.
Adalene: I enjoy partnering with teams across the organization to translate data into meaningful insights that support informed decision-making and ensure stakeholders have the information they need.
Kenneth: My wonderful department. I love being part of this team!
Jennifer Hooks (Actuarial Associate - 14 years starting in 2003, 15 total with ProAssurance): I enjoy getting hands-on with data, both to see it mesh into an output that can be shared with others, as well as to dig around in the details of it when necessary. Anything where there is a question to be answered or a problem to be solved can be a fun exercise.
Jean-Paul: My favorite part of the job is my colleagues. The Actuarial team is fortunate to be replete with an amazing group of people! They always go beyond to assist and support one another.
We asked the team, what is one misconception about your job or the Actuarial department that people often make?
Sokol: That actuaries can tell the future. I am joking of course … but not fully.
A big part of an actuary’s job is setting the price for things that will occur in the future or setting reserves so that the company can make future payments. This requires us to make a significant number of assumptions about the future. Often people associate our number as a “given/certainty,” but everyone needs to understand that the number is based on mathematical/actuarial principles, and very likely future events will be different.
As I often tell people, if I could tell the future I would not need a job as I would be an excellent stock trader!
Bruce: That actuaries aren’t social—communicating data needs and results are key skills.
Glenn: The first thing that is not necessarily a misconception, but may still be relevant, is that a lot of people simply just don’t know what an actuary is or does. Though in fairness, before I decided to get into this line of work, neither did I! But more to the spirit of the question of an actual misconception—that actuary numbers are right. That is to say, even though we do our best and we have strong skills in methods and analyses to try to get to good projections, we are sometimes going to be wrong.
We don’t have a crystal ball. We are just doing the best we can to estimate. So for us, the job is to (a) try to get as close as we can but, more importantly, (b) adjust and react as quickly as possible to make course corrections on those initial projections, especially if it’s clear that maybe we weren’t as close as we would have liked!
Kenneth: People often ask for investment advice because they have the misconception that we review investments.
Jennifer: That we make projections by using some kind of magic or just by guessing!
Jean-Paul: That actuarial work is boring! I often get this remark in most of my nonprofessional gatherings. This misconception likely stems from the technical nature of our work, which involves analyzing data and forecasting future events. However, for those of us who find numbers fascinating and believe that they inherently tell a story, actuarial work is intellectually stimulating and challenging. We must constantly stay updated on industry trends, economic conditions, and regulatory changes. We also play a pivotal role in developing financial strategies, making our work highly engaging and impactful.
Finally, we dug a bit deeper into the data science and asked how states and regions can potentially impact data and data projection.
Sokol: As an actuary your primary responsibility is to project what will occur in the future. Part of that process is understanding how data was generated and if there are unique patterns to it. As such, there are operational patterns that arise in data when you look at each state.
For example, in Florida the majority of policies carry $250K limits. So these losses will behave very differently than, let’s say, in Illinois where most limits are $1M and claims take a significant amount of time to resolve due to the slower nature of the court system.
Due to these facts, Actuarial must take geography into account when making projections.
Tonya: State regulations directly impact claim frequency and claim severity. Noneconomic damage caps, joint and several liability rules, venue regulations, statute of limitations, etc.—each has a significant impact on claim severity, which then directly impacts the cost of providing insurance coverage.
A look at results for the state of Ohio easily demonstrates this link (based on information provided by the U.S. Department of Health and Human Services in their National Practitioner Data Bank, for MDs and DOs in Ohio):
- 1991: Ohio Supreme Court struck down noneconomic damage caps. The next year, claim severity increased by 11.0%. The average annual increase in claims severity (1991 to 1995) was 5.5%.
- 1996: Ohio passed a package of tort reforms. The next year, claim severity increased by 0.1%. Average annual increase in claims severity (1996 to 1998) was 1.4%.
- 1999: Ohio again struck down tort reform. In 2000, claim severity increased by 10.8%, and average annual increase in claims severity (1999 to 2002) was 7.2%.
- 2003: Ohio passed a new package of tort reforms. Claim severity increased by 1.4% for the year, with average annual increase in claims severity (2003 to 2006) at 2.8%. From 2003 to 2009, it was 2.2%.
Bruce: Clean consistent data inputs and consistent company processes, especially claims handling, are vital—and more is better when it comes to data!
Glenn: There actually can be multiple ways regions and states impact how data and data projections work. For example, states have different laws and different legal/litigation environments, and sometimes those can even be different within a given state. States and regions can have different economic conditions, demographics, or cost-of-living standards. All of these can play a role in how much claims will ultimately settle for and, in turn, play a role in how much premium may be charged for a policy.

The Bind Order
This selection of accounts ProAssurance bound recently is intended to give our partners tangible examples of risk classes we’ve been successful quoting and that we’d like to see more of. These examples are anonymized with final premium rounded, but otherwise present actual accounts.
ANESTHESIOLOGY
Maryland
Limits: 1M/3M
Admitted Premium: $10,100
BARIATRICS
North Carolina
Limits: 1M/3M
Admitted Premium: $16,500
PLASTIC SURGERY
California
Limits: 1M/3M
Admitted Premium: $26,800
INTERNAL MEDICINE
Arizona
Limits: 1M/3M
Admitted Premium: $2,400
ASSISTED LIVING
Wisconsin
Limits: 1M/3M
E&S
Premium: $37,000
ASSISTED LIVING
Connecticut
Limits: 1M/3M
E&S
Premium: $25,000
HOSPITAL
North Carolina
Limits: 10M/10M
E&S
Premium: $4,987,500
ORTHOPEDIC SURGERY
Maryland
Limits: 1M/3M
E&S
Premium: $41,300
RADIOLOGY
Indiana
Limits: 500k/1.5M
Admitted Premium: $5,200
PEDIATRICS
Wisconsin
Limits: 1M/3M
Admitted Premium: $12,800
URGENT CARE
California
Limits: 2M/4M
Admitted Premium: $614,800
PEDIATRICS
Connecticut
Limits: 1M/4M
Admitted Premium: $11,400
ORTHOPEDIC SURGERY
Michigan
Limits: 1M/3M
Admitted Premium: $28,400
PAIN MANAGEMENT
New Jersey
Limits: 1M/3M
Admitted Premium: $40,900
BEHAVORIAL HEALTH
Alabama
Limits: 2M/4M
E&S
Premium: $32,000
MEDICAL LABORATORIES
Indiana
Limits: 1M/3M
E&S
Premium: $20,000
BEHAVORIAL HEALTH
Delaware
Limits: 1M/3M
E&S
Premium: $10,500
New Business Submissions
Our standard business intake address for submissions is Submissions@ProAssurance.com. For specialty lines of business, please use one of the following: CustomPhysicians@ProAssurance.com, Hospitals@ProAssurance.com, MiscMedSubs@ProAssurance.com, and SeniorCare@ProAssurance.com. Visit our Producer Guide for additional information on our specialty lines of business.
The types of business and premium amounts are illustrative of where we have written new business and not intended to reflect actual pricing or specific appetites.
.png?width=300&name=MicrosoftTeams-image%20(28).png)
To comply with an order issued by the Florida Office of Insurance Regulation, we will assess premium surcharges on policies written in Florida. The purpose of this surcharge is to secure funds for a regulatory assessment levied by the Florida Insurance Guaranty Association (FIGA), which handles the claims of insolvent property and casualty insurance companies in Florida.
One assessment will be in effect for a total of 1.0% for policies issued October 1, 2025, through September 30, 2026, and recurring until the Series bonds, issued following United Property & Casualty’s insolvency, are no longer outstanding.
West Virginia employs the largest percentage of healthcare workers compared to its total workforce of any U.S. state, according to a new analysis from KFF.
KFF examined May 2024 data from the Bureau of Labor Statistics’ State Occupational Employment Statistics Survey. The survey offers wage and employment estimates by state and industry for research purposes only and excludes self-employed workers.
Nationwide, 12% of workers were employed by ambulatory health care services, hospitals and nursing or residential care facilities. (Becker’s Hospital Review)
Telehealth exploded during COVID. Both physicians and their patients became more familiar with the tool, whereas federal officials made changes and waived barriers so more patients could access care. Today, most emergency waivers have been replaced by state legislation, but because of limited best practice guidelines, state laws differ dramatically. (Medscape)
Between 2013 and 2023, there was a roughly 67% increase in medical malpractice verdicts of $10 million or more, according to data from TransRe. In 2023, the average award in the top 50 medical malpractice verdicts was $48 million, compared to $32 million in 2022.
The awards are meant to help patients and families who have suffered, but much of it can go to other parties involved in the suit. In some states, up to 40% of the award goes to the plaintiff’s attorney, not the plaintiff. A share of the award might also go to the hedge funds and other investors who helped the attorneys pay for the litigation. (Insurance 360)
Large pharmacy benefit managers like CVS Caremark, Express Scripts and Optum Rx are increasingly being blamed for higher drug prices and the outsize role they play in the pharmaceutical supply chain. CVS Health and Cigna, which owns Express Scripts, filed lawsuits last week seeking to stop Arkansas from enforcing a new law that largely prohibits them from owning retail pharmacies in the state. (Axios)
State law mandates that physicians hold at least a 51% stake in most medical practices, but supporters of the new legislation say that companies have taken advantage of a loophole by employing their own physicians and putting their names down as clinic owners, according to the report.
The legislation limits the control companies can have in a clinic’s operations and also bans noncompete agreements that prohibit physicians from taking a position at a different practice, the report said. The bill does not take effect immediately and has a three-year adjustment period for facilities to comply with the new restrictions. (Becker’s Hospital Review)

The Geography of Risk: Why Personalization Wins

You've seen it. Maybe you've even done it: Selling to every healthcare provider like they're all the same. Same pitch. Same story. Same assumptions. Because obviously, every Ob-Gyn lies awake dreading shoulder dystocia lawsuits. Every cardiologist is haunted by a missed ECG reading. And every orthopedic surgeon's biggest fear is operating on the wrong leg.
It's easy to think you've found the formula: pair a known risk with a specialty and run with it.
Except, it doesn't work.
Sure, you'll get some bites, but you're also helping prospects commoditize your risk coverage—or worse— giving them the impression it's the wrong fit.
Doctors might share a specialty, but they don't share a brain. Every physician—and the practice manager whispering in their ear—has their risk tolerance, pain points, biases, experiences, and, yes, state regulations shaping how they see coverage. It's worth repeating the Stan Starnes (ProAssurance’s former CEO) quote: "If you're in 50 states, you're in 50 different lines of business," and each expects you to speak their language.
MPL: It's Personal—Right Down to the Zip Code
Every healthcare provider knows they need protection from liability—but it doesn't hit home until they see themselves in the risks you're describing. That's why effective MPL selling isn't just about explaining coverage—it's about making it palpable. Personalize everything: the stories you tell, the case studies, the policies. This isn't just about the physician but also the practice, the decision-makers behind the scenes, and the state(s) where they operate because that's where the real risk lives.
It's reality. A family practice doctor in Indiana doesn't think like a plastic surgeon in Beverly Hills. The risks, concerns, and even how they buy coverage are different. And if you're proposing coverage for a physician in New York the same way you'd pitch someone in Tennessee, all you're doing is shifting from digital spam to delivering it live.
Personalizing by State Isn't Just About Regulations
When you walk into a client meeting without knowing the local risks, laws, or recent headlines shaping how that doctor sees liability, what message are you sending? You're saying: “I didn't care enough to prepare.” And if you didn't care enough to do that, why should they care enough to listen?
Prospects expect you to understand their liability risks and the regulatory landscape. But when they sense you know their practice, concerns, and local exposure better than anyone else, you don't just stand out—you move to the top of their list.
Real-Time, Relevance-Based Selling: Your Secret Weapon
Want to rise above every other agent pitching the same prospects? Focus on what matters to them right now.
Real-time, relevance-based selling refers to identifying immediate concerns—and positioning the best options. That might mean discussing rising verdict sizes in their county. Maybe it's reviewing why their locums coverage exposes them in multiple states. It could mean knowing their hospital just got sued—and helping them avoid the same trap.
If you can position your policy perfectly—for them, their practice, their region, right now—they'll see why you're the obvious choice.
Do the Work. Get the Win.
Selling across state lines isn't just a change in scenery—it's a change in strategy. Each state has its own legal landscape, medical culture, and decision-makers. That means tailoring your approach to each prospect's specialty, practice dynamics, way of thinking, and local risks.
When you take the time to dig in and speak to what matters most, you stop being just another agent with a quote and start becoming the trusted resource they've been waiting for. With ProAssurance behind you—offering tailored options in every state—you're equipped to deliver what today's buyers expect.
Fifty states. Fifty different games. Play each one like you came to win.

|
Written by Mace Horoff of Medical Sales Performance. Mace Horoff is a representative of Sales Pilot. He helps sales teams and individual representatives who sell medical devices, pharmaceuticals, biotechnology, healthcare services, and other healthcare-related products to sell more and earn more by employing a specialized healthcare system. Have a topic you’d like to see covered? Email your suggestions to AskMarketing@ProAssurance.com. |

Risk Management June Releases
2025 Practice Administrator Seminar Now Live
This year’s topic is “Connectivity with Caution: Digital Communication Essentials for Practice Managers.” This seminar is intended for practice administration professionals and medical office staff working within all physician specialty groups. There are no required experiential or academic prerequisites.
Program Description
Technology allows physician office practices to communicate with patients across multiple platforms including electronic health records, text messaging, patient portals, and social media. This program will review patient scenarios, provide risk mitigation strategies, and address the risk related to digital communication with patients and other healthcare professionals.
Objectives
This educational activity will support one’s ability to do the following:
- Evaluate and mitigate the risks of digital communication tools used in the delivery of care.
- Apply risk reduction strategies to reduce potential patient harm and professional liability claims.
Promoting the Seminar
A promotional mailing for this seminar will go out in early July to eligible insureds. We will also send copies of the mailing to our agency partners as a reference should you have questions or receive questions from your clients.
The Allegation
Patient’s family alleged that the radiologist failed to communicate abnormal post procedure chest x-ray results to the ordering interventional radiologist.
Read MoreProAssurance recognizes communication as a critical aspect of a positive patient experience. Working to bridge the gaps across different languages and communities is a piece of that experience.
Watch VideoIn this episode, the importance of informed consent, the ethical implications of patient autonomy, and the necessity of thorough documentation when patients refuse care is discussed.
Read MoreImportant Notice Regarding the Certitude Program
After more than a decade of providing a program for coordinated defense for Ascension-affiliated physicians, Ascension and ProAssurance have agreed that the Certitude program will begin winding down on October 1, 2025. This decision was reached due to the changes in the availability of the program and changes for Ascension-owned ministries.
ProAssurance will be informing insureds of the change ahead of the required notice for material changes. We will share this information ahead of each renewal date. Please share this information among your agency teams as well.
Regardless of the discontinuance of the Certitude program, your clients’ current policies remain in effect with no changes to any element of coverage or service through its expiration date. The only change is, at the current policy’s expiration date, your clients will be offered a renewal policy by ProAssurance but not a renewal policy under the Certitude Purchasing Group program.
If you have any questions regarding the change, please contact your Business Development representative.
ProVisions Team
- Communications
- Design
- Digital Marketing










