















|
|

|
|



Dr. Jekyll Unmasked in the OR
A terrifying tale of mental health meeting malpractice ...
The surgeon … to everyone’s unbelieving horror—began operating as though in a world gone mad. He was in Cantrell’s obese body within about a minute, had the gallbladder out in two or three minutes more, and was beginning to dissect the stomach, not bothering to tie off any but the largest vessels, leaving the smaller ones to spurt bright red arterial blood onto the drapes and over the masks of the assistants. Before I realized how far he’d gone, he tossed a perfectly normal section of the stomach into a specimen pan and—right before our astonished eyes—cut a transverse slash though the front wall of the aorta. The decibel level in the room rose as high as the column of blood blasting its lethal way toward the ceiling …
That was a scene from Dr. Sherwin B. Nuland’s collection of medical tales, The Soul of Medicine: Tales from the Bedside. The story, told by the anesthesiologist present, goes on to explain that this once competent and dependable general surgeon was also—unknown to most at the hospital—under medication for a chronic mood disorder. He had just returned from a three-week vacation, which included a vacation from taking his meds.
The patient not only survived but thrived. He had struggled with obesity and, while this incident preceded modern bariatrics, the stomach repair functioned similarly to surgical stapling resulting in a trim new body that he retained for the remainder of his life. The repair to his aorta was sound, never causing a complication. The billing for the gallbladder removal (the reason he was in for surgery) was waived and, after the numerous lawsuits settled, the 55-year-old accountant never had to work again!
A Decade On, Our Retention Program Is Frighteningly Strong
Earlier this year I read The Soul of Medicine, a potential candidate for the “response offer” for our annual customer retention campaign. For more than a decade, our practice has been to mail physician insureds a thank-you note for choosing ProAssurance. These direct mail pieces are sent to physicians written in the standard market in small- or medium-sized groups approximately 90 days in advance of their renewal. The direct mail pieces include a response offer. If the insured returns the enclosed postcard, we mail them the selected item at no additional cost.
Because the offer is usually a book, we review a lot of titles to decide whether they might be good for the campaign.
The books we are seeking typically fall into one of three categories:
1. Doctors writing about being doctors: In past campaigns we offered Attending by Ronald Epstein, MD (in 2018), and last year was The Laws of Medicine by Siddhartha Mukherjee.
2. Risk management or patient safety: Dr. Danielle Ofri is a terrific resource in this category, and we’ve used two of her books: When We Do Harm in 2023 and What Patients Say, What Doctors Hear in 2020.
3. A current event or trend affecting medicine: In 2023 we got ahead of the AI wave before ChatGPT went mainstream by offering Eric Topol’s Deep Medicine. In 2021, a year after the pandemic financially stressed medical practices, along with most other businesses, our response offer was Dr. James M. Dahle’s The White Coat Investor. Jim spoke that year at our agents’ Leadership Elite annual meeting in Park City, UT.
This year’s campaign offer is When Good Doctors Get Sued by Angela M. Dodge, PhD. This aligns with our marketing push to both highlight the rising claims severity crisis and differentiate ProAssurance as having the most capable Claims department in the medical malpractice industry. This title is also recommended by Dr. Gita Pensa, a leading physician litigation stress advisor. Our Risk Management department partnered with her this year on a variety of projects, including her Physician Online Seminar, “Healing the Healers: Litigation Stress Support for Physicians,” and a guest appearance in an upcoming episode of our Rapid Risk Review podcast.
We target a 20 percent response rate for these campaigns and see anything above 25 percent as an excellent year. After the campaign, we compare the renewal rates of responders to non-responders. While correlation is no causation, the higher rate of renewals among the responders leads us to believe the benefit exceeds the time and costs to run the campaign. So far in 2025, we are running a little behind, but the year is not over yet, and we’ve been experimenting with changes to try to increase responses along the way. The slow 2025 may simply be a less popular book choice (mine). Despite nuclear verdicts in the headlines, I fear insureds just don’t think it will happen to them—until it does.
The response offers have not always been books. Back when thumb drives were useful but not yet considered vectors for malware, we offered a Risk Management Resource Kit. Another year we used the campaign to promote our cyber-insurance buy-up product, ProSecure, by sending out webcam covers with the mailers, before embedded covers became standard on most laptops.
Our plan for 2026 is not only “not a book,” but it’s also an internal Risk Management team creation. We’re always seeking new ways to bring risk management issues to the attention of our insured physicians and practice managers. This year’s new podcast, Rapid Risk Review, is an example, as is our long-running YouTube series, “2 Minutes: What’s the Risk?” We’ve heard about practice managers kicking off staff meetings by showing one of our short videos. As another tool in that spirit, our Risk consultants created a set of conversation starter cards called “What’s the Risk?” Conversation Cards. Each card in the set has one question on it designed to engage practice staff in a discussion about one specific operational risk management topic. The set of cards is laminated on heavy card stock with a hole in the corner and bound together on a ring. We field-tested these at the ASHRM conference in Charlotte last month. The feedback was positive enough to convince us it should be next year’s response offer.
 If you’d like a sample of the 2025 book, campaign materials, or next year’s Conversation Cards, just let us know by contacting Marketing at AskMarketing@ProAssurance.com. Include your name, the items and quantities you’d like, and the mailing address.
If you’d like a sample of the 2025 book, campaign materials, or next year’s Conversation Cards, just let us know by contacting Marketing at AskMarketing@ProAssurance.com. Include your name, the items and quantities you’d like, and the mailing address.

- Risk Management Team
















.png?width=300&name=MicrosoftTeams-image%20(28).png)

When the Rush Becomes the Risk
Some people get their fright fix from haunted houses at Halloween. Others prefer a more realistic experience, such as one that comes from speed.
When I was 15, my friend Billy invited me for a ride to show off the Pontiac Grand Am he and his dad had rebuilt. He warned, “Buckle up tight!”
The engine practically begged to run. Moments after turning onto Jericho Turnpike, with the nearest car at least a mile down the road, Billy punched the accelerator, pinning me to my seat. The speedometer climbed—90, 110, 140. I remember screaming, “Slow down!” as telephone poles blurred by. It’s a fun memory and one I’m glad to have survived.
A decade later, I learned about speed in another place where it can either save lives or cause harm—the operating room.
I’ve stood beside trauma teams when every second mattered. I’ve also witnessed medical professionals who rush out of habit instead of medical necessity.
Let’s Go
I worked with a surgeon who craved speed just as Billy did. Dr. Speedy, as he was known, burst through the OR doors for every case with his trademark greeting: “Let’s go!” His cases were a surgical sprint, and he quickly sidelined anyone who couldn’t keep up.
Speedy often performed unicompartmental knee replacements, which required ordering the exact side and compartment in advance. Because his staff scheduled cases with hurried phone calls, I required them to fax the implant details for every uni knee to protect myself, and I kept each fax in a binder for proof.
One day, while I was covering another hospital, Speedy’s OR called in a panic: “You sent the wrong implants. Can you get us the right ones, stat?” I couldn’t; my company had shipped exactly what they ordered. His only option was to do a total knee replacement, and he immediately tried to blame me. Thankfully, my binder of faxed orders spoke louder than his accusations, showing the mistake came from his office.
I had repeatedly witnessed the true villain in his practice—the doctor fueling a rushed environment where details fell through the cracks.
Too Many Real-World Horror Stories
Dr. Speedy’s patient did fine—switching to a total knee was still within the standard of care. But not every story ends well. Across healthcare, mistakes linked to a “speed mentality” happen more often than anyone would like to admit.
Case studies where rushing led to ignoring safeguards are not uncommon: Teams that hurried through—or skipped—the mandatory time-out to confirm patient and procedure; surgeons who bypassed critical imaging or visualization before inserting a trocar or making an incision; and production pressure, packed schedules, or last-minute emergencies that pushed entire operating rooms past the margin of safety.
What MPL Agents Can Take Away
For MPL agents, these stories are more than cautionary tales. They’re conversation starters with physicians who value efficiency but must also consider potential trade-offs. Use them to highlight:
- The hidden accelerants: packed schedules, staffing gaps, and throughput pressures that tempt teams to skip verification.
- The shield of documentation: policies and procedures—and the malpractice coverage that backs them—are only as strong as the records behind them.
And from a sales or business perspective? The lesson is the same. Rushing a prospect or client visit, skipping discovery questions, or failing to confirm details is the business equivalent of malpractice. Consider a “time-out” before proposing coverage options. Pause to confirm the risks, the decision-makers, and their genuine concerns. And yes—keep impeccable notes.
The rush of speed can be exhilarating, but unlike a haunted house, there’s no exit sign when urgency steamrolls protocol. Let’s help HCPs limit the scary moments in healthcare.

|
Written by Mace Horoff of Medical Sales Performance. Mace Horoff is a representative of Sales Pilot. He helps sales teams and individual representatives who sell medical devices, pharmaceuticals, biotechnology, healthcare services, and other healthcare-related products to sell more and earn more by employing a specialized healthcare system. Have a topic you’d like to see covered? Email your suggestions to AskMarketing@ProAssurance.com. |


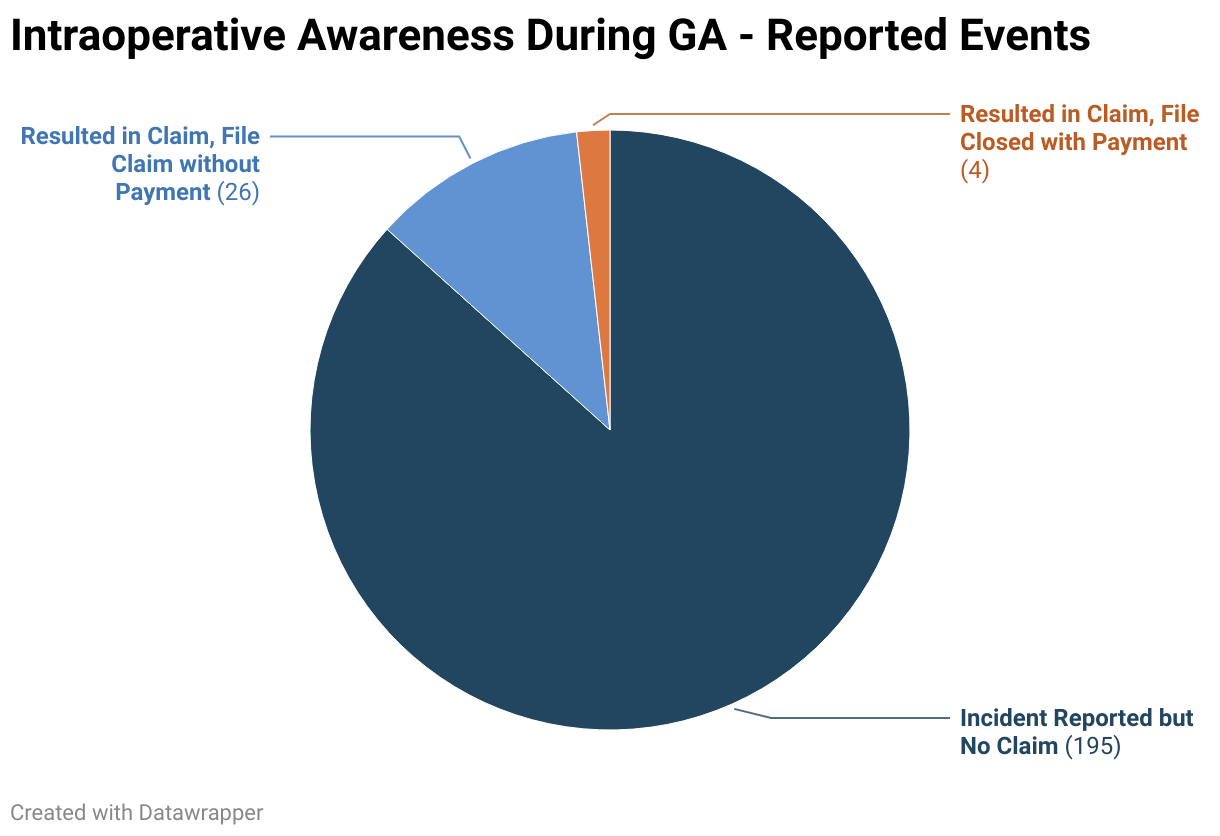
Event reporting is a systematic and timely internal process of reporting occurrences that deviate from expected outcomes. Adverse events include medical errors, near misses, and patient harm obtained as the result of the care delivering process. The benefit of event reporting is to foster a culture of patient safety and provide the opportunity for process improvement.
Watch here
Allegation
The parents of a 3 YOF alleged that pediatricians failed to properly and timely diagnose and treat the patient’s bronchopneumonia via telemedicine and in person, resulting in her death.
Read the issue

Spoliation is the intentional or unintentional destruction or loss of evidence that may be used in connection with litigation. Learn how spoliation can happen and what you can do to avoid finding yourself the subject of a spoliation jury instruction during a medical malpractice claim.
- Communications
- Design
- Digital Marketing










