








.png?width=300&name=MicrosoftTeams-image%20(39).png)
It can be a difficult balance treating patients’ pain while also taking crucial steps to avoid misuse, abuse, dependence, and overdose of opioids. Providers must recognize “red flags” and signals of misuse, abuse, or dependence. In the context of treatment for chronic pain, addictive behaviors may be difficult to identify. That’s why we’ve partnered with Sure Med Compliance. Their mission is to end the overdose epidemic through greater prescribing compliance by offering the first and only digital health platform scientifically validated to mitigate risk to both patient and provider in pain management settings.
By delivering clinical insights that help influence safer prescribing decisions, Sure Med helps protect healthcare providers from liability and allows doctors to create safer exposures to controlled substances.
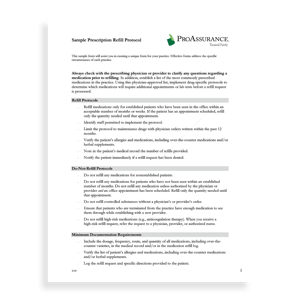
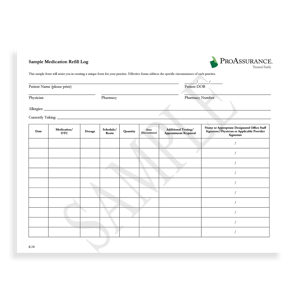
They recognized a point-of-care problem: To initiate or continue controlled substance therapy legally, a physician must determine and document up to 26 data points in a 5- to 10-minute office visit. This may not be feasible for busy doctors, so it may not get done. The unintended consequences may lead to poor outcomes and provider liability.
With Sure Med’s digital health platform, the patient is evaluated electronically, and the results are delivered immediately to their Electronic Health Record. This eliminates 80% of the time needed to determine and document the necessary data points to initiate or continue controlled substance therapy.

Through our exclusive affiliation with Sure Med, ProAssurance is at the forefront of helping physicians to prescribe more responsibly, leading to better outcomes for patients. We encourage your clients who regularly prescribe opioids, especially those who prescribe for chronic pain, to learn how Sure Med can help them develop and maintain safe and responsible prescribing practices, which in turn, should lead to better outcomes for their patients.
By partnering with companies dedicated to new technologies and innovation that benefit patients and improve lives, ProAssurance is able to facilitate reducing provider risk and ultimately protect others. It is an intersection of potential that aligns with our purpose.
Learn More: SureMedCompliance.com
SEMINARS
The ProAssurance Risk Management team offers several seminars focusing on prescribing opioids, including keeping a physician’s patient safe, risk management regarding opioids, and the most recent CDC guidelines for prescribing opioids for chronic pain. These seminars take a longer amount of time, but physicians can earn CME credits once they successfully complete a seminar and pass the posttest with a score of 75% or greater. All the seminars take roughly an hour to complete, and they are located on Risk Management’s seminar page.


OPIOID PRESCRIBING
The Tragic Toll of Opioid Abuse in America
In 2020 (the latest year for which CDC data are available), 16,416 Americans died of prescription opioid-involved overdose — a 16% increase over 2019 and the first increase since 2016.1,* This despite decreases in both total prescriptions (-6.8%) and prescribing rate (-3.4 points).2,† It’s no surprise, then, that overdose death involving opioids is referred to as a public health emergency and an epidemic.3
Although the death rates‡ for prescription opioid overdose are lower than death rates for synthetic opioids — over which healthcare providers have little direct influence — research seems to indicate that some patients who abuse prescription opioids will at some point transition to illicit opioids such as fentanyl and heroin.4 Consequently, there are good reasons for opioid prescribers to remain vigilant about carefully balancing the risks and benefits of opioid therapy for chronic pain.
A review of our closed claims indicates that claims involving opioid therapy in chronic pain management patients generally involve overdose deaths. Allegations supporting negligence claims against physicians include excessive opioid prescribing; failure to refer the patient for pain management, addiction, or behavioral health treatment; failure to discover the patient was doctor shopping; failure to recognize suicide risk; and negligent tapering.


THE PATH FORWARD
The case studies in our Knowledge Library use closed claims, policyholder inquiries, and medical board actions to identify pain management best practices “that balance a focus on optimizing function, quality of life (QOL), and productivity while minimizing risks for opioid misuse and harm.”5
CONCERNS
- 21-29% of patients prescribed opioids for chronic pain misuse them.6
- 8-12% of patients prescribed opioids for chronic pain develop an opioid use disorder.6
CHALLENGES
- Clinicians are responsible for the safety of the patients for whom they prescribe opioid pain medications.
- There are no shortcuts to reducing the risk of accidental and intentional overdose.
- Misinterpreted and misapplied prescribing guidelines can cause patients to turn to illicit drugs like fentanyl or heroin to manage their pain and withdrawal symptoms.5
STRATEGIES
- Develop pain treatment plans that balance optimizing function, quality of life (QOL), and productivity while minimizing risks for misuse and harm.
For more information and links to case studies and risk reduction strategies—as well as notes and numbered references—visit our Knowledge Library article “Opioid Prescribing for Chronic Pain: Case Studies and Best Practices.”

 As the opioid epidemic continues to plague the healthcare industry, it presents a unique challenge for healthcare professionals, particularly physicians, who are often torn between their duty to alleviate pain and the risk of legal consequences, even imprisonment. It also creates a challenge for MPL agents who recognize the importance of including discussions about opioid liability as a regular part of sales conversations with prospects and clients. Opioids are a hot topic with physicians and will likely get their attention. The challenge is that doctors often avoid or dismiss discussions they perceive as sales pitches, especially if they believe they’re already managing the risks involved.
As the opioid epidemic continues to plague the healthcare industry, it presents a unique challenge for healthcare professionals, particularly physicians, who are often torn between their duty to alleviate pain and the risk of legal consequences, even imprisonment. It also creates a challenge for MPL agents who recognize the importance of including discussions about opioid liability as a regular part of sales conversations with prospects and clients. Opioids are a hot topic with physicians and will likely get their attention. The challenge is that doctors often avoid or dismiss discussions they perceive as sales pitches, especially if they believe they’re already managing the risks involved.
For instance, if you try to initiate a conversation with a physician about the importance of liability coverage when prescribing opioids, the doctor may balk if they already follow the Centers for Disease Control's (CDC) Clinical Practice Guideline for Prescribing Opioids for Pain. They may also feel that their current medical professional liability (MPL) policy is sufficient. However, it can be more difficult for physicians to ignore an opportunity to learn how their colleagues manage similar risks. By opening a meeting with concrete examples and demonstrating your expertise, you may gain the physician’s attention and interest, and engage them in a meaningful discussion.
One of the best ways I’ve found to avoid the typical HCP response of "I'm happy with my current product” is by opening with a technique I call SCY that shifts the initial focus away from the sale.
SCY stands for Situation / Colleagues / You:
Situation: Describe a situation the prospect has or is likely to encounter.
Colleagues: Describe how the prospect’s medical colleagues commonly respond in that situation.
You: Ask the prospect, “What do YOU do in this situation?”
One key aspect of the SCY approach is that it centers the conversation on the physician's expertise and clinical approach. This helps to establish a more genuine and meaningful dialogue rather than simply trying to pitch a product or service. Here is an example of how the SCY method could open a discussion: "Prescribing opioids to patients with a history of abuse is a potential liability issue. Some of your internal medicine colleagues prescribe only the minimum dosage for the shortest duration, whereas others won’t prescribe opioids to these patients and refer them to a pain management specialist instead. What do you do in this situation?”
You'll initiate a more personalized conversation by introducing a specific circumstance and asking for the prospect's opinion instead of merely giving a product-focused sales pitch. The SCY approach can be particularly practical because it allows you to learn what is most important to the prospect in a given situation or context. When you transition to discussing appropriate strategies or coverage options, you can tailor the benefits you present to the prospect’s specific concerns. This is a more compelling approach than simply reciting a list of benefits and hoping that some of them resonate.
As the clinical and legal landscape around prescribing opioids evolves, you will have ongoing opportunities to provide value to physicians by sharing strategies for managing the risks associated with this class of drugs. The SCY technique can be a helpful tool for starting a personalized and comfortable conversation about the challenges of prescribing opioids and for helping doctors understand the importance of staying current with best practices and obtaining adequate (MPL) coverage.

Written by Mace Horoff of Medical Sales Performance
Mace Horoff is a representative of Sales Pilot. He helps sales teams and individual representatives who sell medical devices, pharmaceuticals, biotechnology, healthcare services, and other healthcare-related products to sell more and earn more by employing a specialized healthcare system.
Have a topic you’d like to see covered? Email your suggestions to AskMarketing@ProAssurance.com.
.png?width=300&name=MicrosoftTeams-image%20(28).png)



We are pleased to announce that Tori Warsko has joined ProAssurance as Business Development Representative for the Southwest Region, effective January 9, 2023.
Tori comes to us from Wolverine Mutual Insurance Company where she acted as Territory Manager for the entire state of Indiana and the southwest region of Michigan. She has extensive experience working with principals and producers to identify business obstacles, establish financial goals, and tailor products to individual markets. She earned her bachelor’s degree in Business Administration from Ferris State University.
You can reach Tori directly at 205-776-3066 or ToriWarsko@ProAssurance.com.
.png?width=300&name=MicrosoftTeams-image%20(13).png)
We are pleased to welcome Anthony (Tony) Peterson to ProAssurance, where he will serve as Assistant Vice President of Business Development for the Southeast Region, effective January 30, 2023.
Tony has more than 30 years of MPL industry experience and is skilled in developing and managing complex risk and insurance programs. He comes to us from MagMutual Insurance Company, where he was Vice President of Business Development and responsible for the growth and retention strategy for hospitals and healthcare systems across the U.S. He has extensive strategic leadership experience and a talent for developing and maintaining trusted relationships with key agent/broker partners. He attended DePaul University, College of Business, and holds the Associate in Risk Management (ARM) designation from the American Insurance Institute.
You can reach Tony directly at AnthonyPeterson@ProAssurance.com.
.png?width=300&name=MicrosoftTeams-image%20(12).png)
